Patterns of access to Cardiac Magnetic Resonance imaging in the Riverina
Dr Su San Lim, A/Prof Joseph Suttie
Introduction
Cardiac Magnetic Resonance imaging (CMR) has become a valuable diagnostic tool for cardiac conditions. It is the imaging modality of choice for complex congenital heart disease, and particularly useful for diagnosing structural conditions including cardiomyopathies, inflammatory and infiltrative conditions.
CMR imaging first became available in Wagga Wagga in 2013, increasing access to patients in the Riverina who face geographical difficulties in travelling to the city.
Objectives
To evaluate and describe local patterns of access to CMR, and compare the rates of uptake between residents in Wagga Wagga and peripheral towns.
To evaluate level of accessibility to CMR amongst Indigenous patients in the Riverina.
Methods
Retrospective data of 202 patients who had CMR imaging was collected over 5 years from 2013-2017 at the main referral centre, Riverina Cardiology.
Variables analysed included age, sex, distance travelled, Indigenous status and year of presentation.
Results:
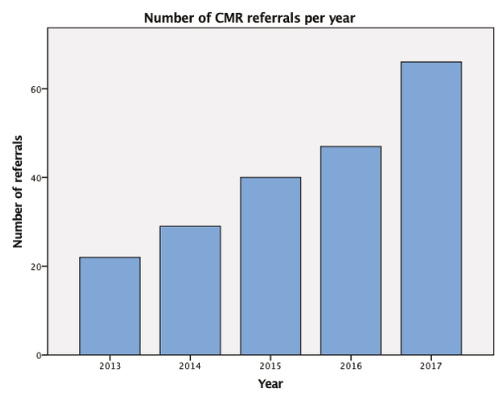
The number of patients accessing CMR has steadily increased over the years since it first became available (Figure A).
The main indications for referral included investigation of cardiomyopathies, masses, arrhythmias, valvulopathies and ischaemic heart disease.
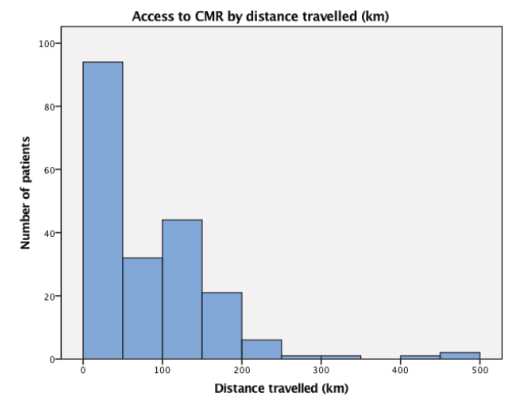
Rates of access increased with lesser distance required to travel (Figure B). Out of a total of 202 patients, 81 (40%) lived in Wagga Wagga within 15km of the imaging centre. The remaining 121 (60%) lived in peripheral towns beyond 15km of the imaging centre, with the largest number of patients from Young, Tumut, Temora and Griffith.
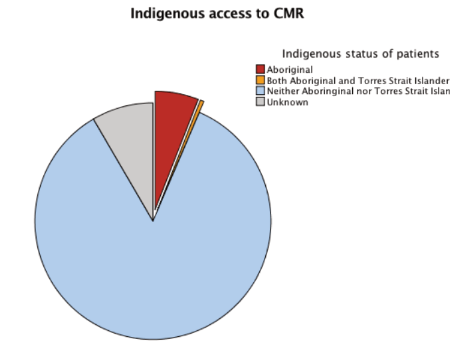
In terms of Indigenous status, the majority of the patients were non-Indigenous (85.4%), 6.4% of the patients were Indigenous, and the remaining were unrecorded (Figure C).
 (a)
(a)
 (b)
(b)
 (c)
(c)
Conclusions
These results show an encouraging yearly trend of increasing regional access to CMR. A larger proportion of our patient cohort live in peripheral towns, showing that the service has reached a population that faces larger barriers to access from geographical and socioeconomic factors.
Indigenous patients are currently slightly over-represented (6.4% scanned population and 4% in the Riverina as a whole). This might represent a higher prevalence of cardiac disease or improved access due to “Close The Gap” financial initiatives designed to improve patient access.
Given the diagnostic benefits of CMR imaging, ease of access should be increased by de-centralising CMR referrals from cardiologists to other clinicians.
Limitations of this study include difficulties in measuring patient adherence to referrals, loss to follow up, and access to GPs and cardiologists.
Further studies should follow to evaluate the benefits from our local CMR service, in terms of diagnosis and treatment of cardiac conditions, so as to help promote funding of other similar CMR services in regional Australia.
References
1. Florian von Knobelsdorff-Brenkenhoff, F and Schulz-Menger, J. (2016). Role of cardiovascular magnetic resonance in the guidelines of the European Society of Cardiology. Journal of Cardiovascular Magnetic Resonance.18(6). DOI 10.1186/s12968-016-0225-6