Navigating Risk-Based Skin Check Intervals for incidentally found Keratinocyte Carcinomas in a Targeted Melanoma Screening Project
Neeraja Thirukkumaran1,2, Amelia Smit3, Maria Paula Senna4, Bruna Gallo1, Gabriella Parsons2, Methmi Perera5, Terence Wong1,5, Serigne Lo1,5, Pascale Guitera1,5, Bruna Gouveia1, Christoph Sinz1, Anne Cust*1,3, Linda K Martin*1,2,3
*Joint final author
Affiliations: Melanoma Institute Australia, University of New South Wales
1. Melanoma Institute Australia,
2. School of Clinical Medicine, Faculty of Medicine & Health, UNSW Sydney, Australia
3. The Daffodil Centre, The University of Sydney, a joint venture with Cancer Council NSW, Sydney, Australia.
4. IDOMED — Estácio de Sá University, School of Medicine, Rio de Janeiro, Brazil
5. Faculty of Medicine & Health, The University of Sydney, Australia
Introduction:
The need to establish evidence-based skin cancer screening is paramount. Risk-stratified intervals has potential to improve efficiency, cost-effectiveness and minimize unnecessary healthcare resource strain.
Aims:
To assesses screening appointments (SA) per keratinocyte carcinomas (KC), incidentally diagnosed in the ‘Tailored Surveillance’ targeted melanoma screening project.
Methods:
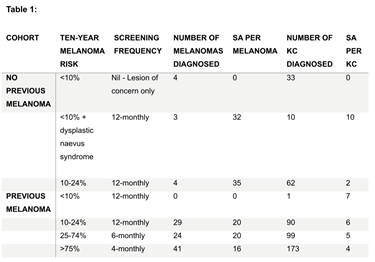
A prospective cohort study was conducted from 08/02/2021 to 31/07/2022 with follow up until 31/07/2023. Prospective risk-stratified skin check intervals were implemented, and through retrospective clinical record review, screening appointments for melanomas and KC were analysed. Study eligibility included ≥18 years old, English-proficient, and minimum 12-months follow-up. Participants undertook an online risk-assessment which provided skin-check frequency recommendations based on estimated melanoma ten-year risk (Table 1).
Results:
This study had 591 participants with primary cutaneous melanomas (n=102) diagnosed in 75 patients during the follow-up period. 458 KCs (339 BCCs and 119 SCCs) were diagnosed with the recommended SA/melanoma and SA/KC displayed in Table 1.
Conclusion:
This study explores risk-stratified screening intervals in a melanoma project and the incidental detection of KCs during follow-up. KCs do not qualify for screening due to rare fatality, yet overlapping risk factors with melanomas will undoubtably result in identification during melanoma screening. Diagnosis and treatment of KCs are likely to inflate melanoma screening costs. Whilst early detection may reduce morbidity, there remains a risk of unnecessary treatment of indolent tumours. This can help guide a national screening program.